What is Pocket Brain? I How to I Index I References I EN – DE – IT – ES – FR – RU – CN
Normal brain at midgestation: axial views
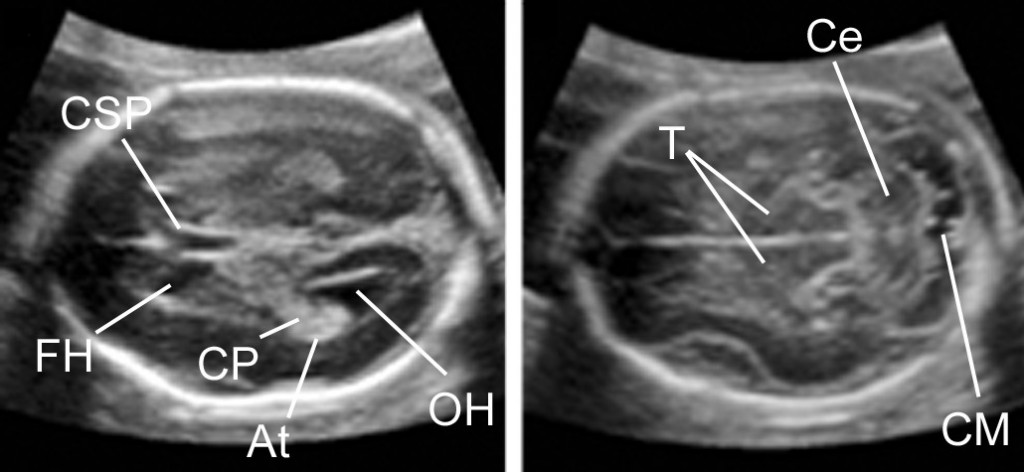
At, atria; B, body of lateral ventricle; CC, corpus callosum; Ce, cerebellum; CeV, cerebellar vermis; CM, cisterna magna; CP choroid plexus; CSP, cavum septi pellucidi; FH, frontal horns, OH, occipital horns; TH, temporal horns
The two sections shown above, the transthalamic and the transcerebellar view, constitute the brain screening exam. Further views are part of the extended fetal neurosonogram. ISUOG CNS Screening Guidelines I Lecture
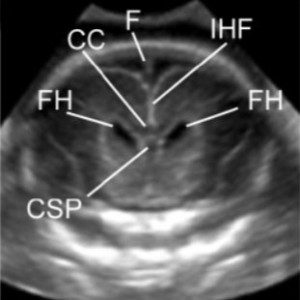
Normal brain: coronal views (back to top)
Normal brain at midgestation: sagittal views (back to top)
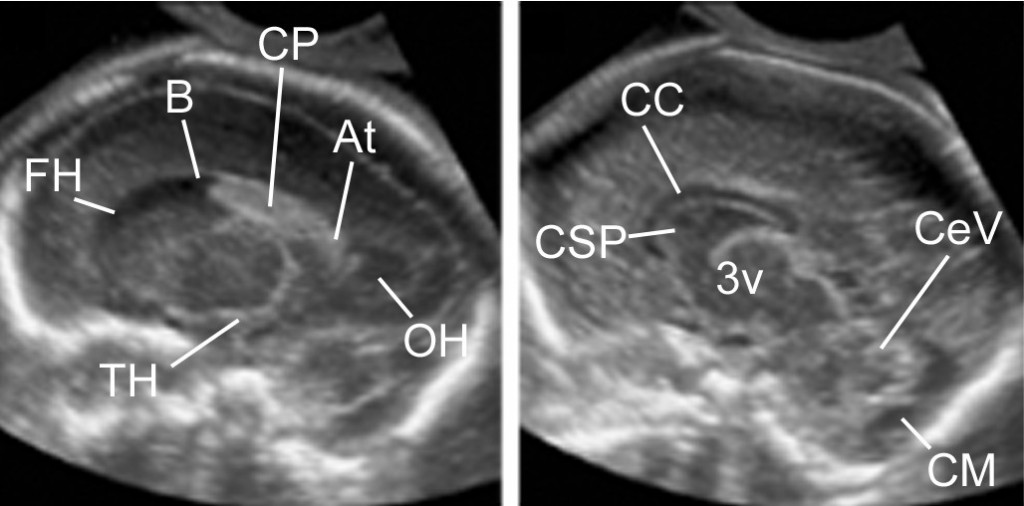
At, atria; B, body of lateral ventricle; CC, corpus callosum; Ce, cerebellum; CeV, cerebellar vermis; CM, cisterna magna; CP choroid plexus; CSP, cavum septi pellucidi; FH, frontal horns, OH, occipital horns; TH, temporal horns
Normal spine I back to top I Index
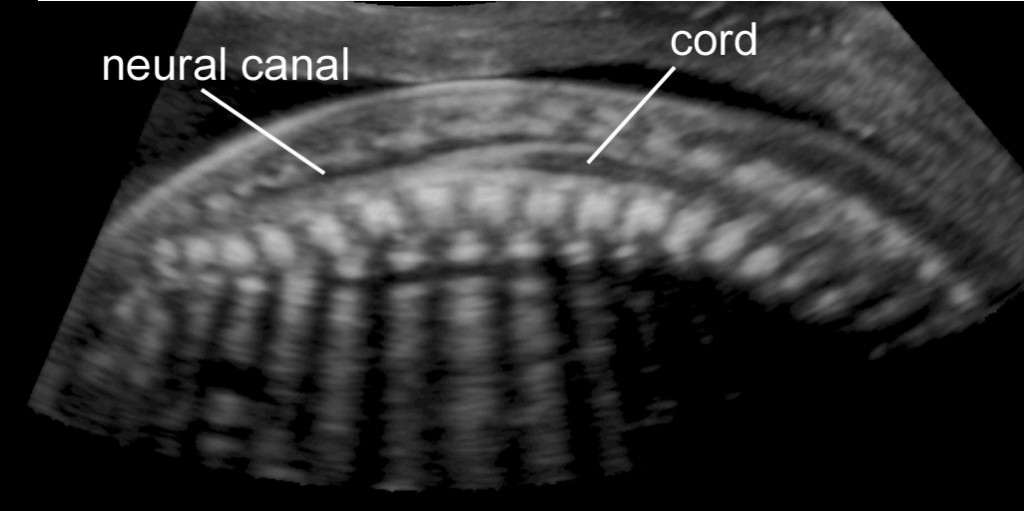
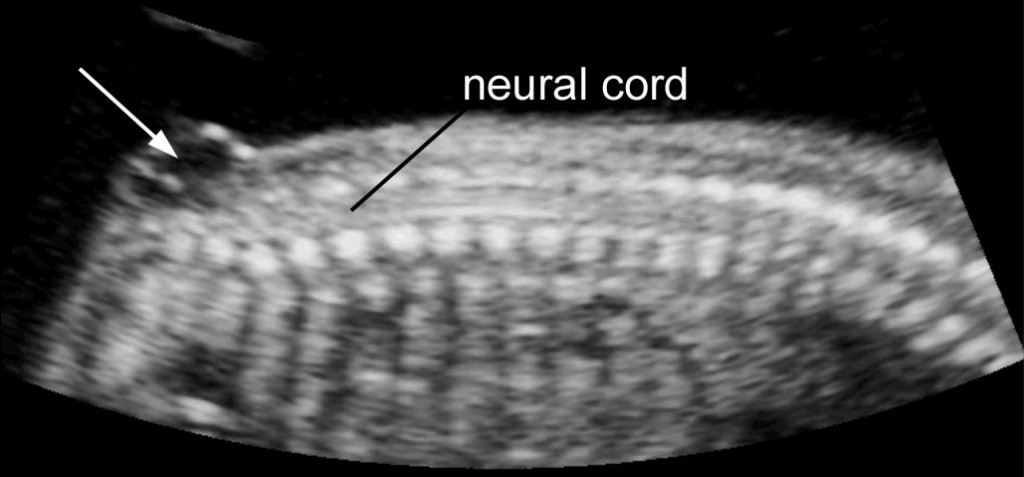
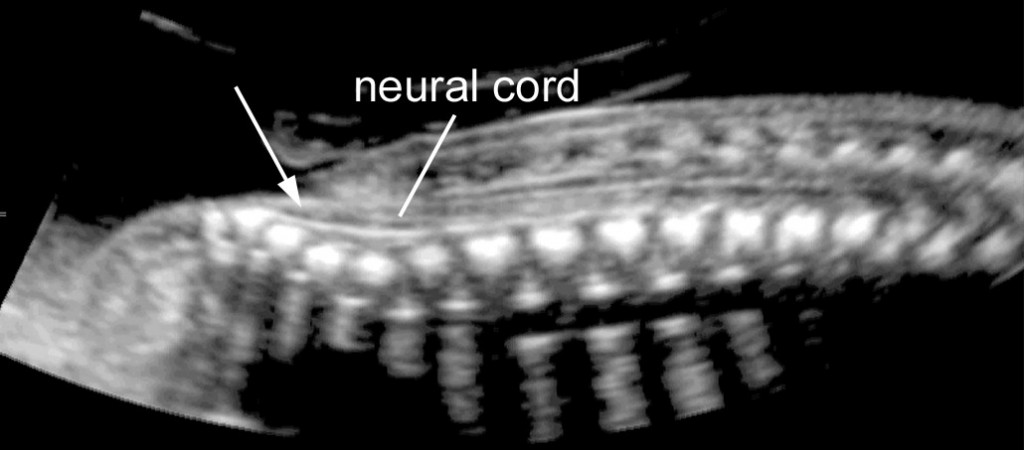
Normal spine at midgestation: Sagittal view demonstrating the ossification centers of the spine, the integrity of the neural canal and the spinal cord. VISUOG I Lecture
Isolated ventriculomegaly I back to top I Index
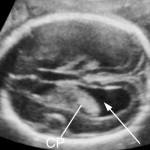
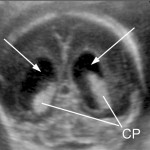

Ventriculomegaly (VM) can accompany different brain pathologies. Isolated VM is a diagnosis of exclusion. The arrows indicate the distended lateral ventricles. VISUOG I Lecture
Anencephaly (late first trimester) I back to top I Index
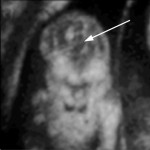
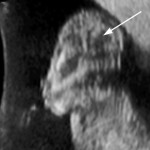
The calvarium is absent and distorted brain tissue (arrow) is seen arising from the skull base and floating in the amniotic fluid. VISUOG
Spina bifida I back to top I Index
Myelomeningocele in a midtrimester fetus (sagittal view): In the sacral area the neural canal is open and communicates with a septated cystic mass (arrow); the spinal cord can be seen extending much lower than usual reaching the level of the defect. VISUOG I Lecture
Myelocele in a midtrimester fetus in sagittal view: In the sacral area the neural tube is open and exposed to the amniotic cavity without an interposing cystic structure. The sagittal plane demonstrates that the spinal cord reaches the level of the defect. VISUOG I Lecture
Arnold-Chiara malformation (cranial signs of spina bifida) I back to top I Index
Arnold-Chiari malformation in a fetus with open spina bifida: There is frontal bossing (also referred to as lemon sign) (arrows); the cerebellum (Ce) is poorly delineated because of the absence of fluid in the cisterna magna (also referred to as banana sign).VISUOG I Lecture
Holoprosencephaly, alobar (13 weeks‘ fetus) I back to top I Index
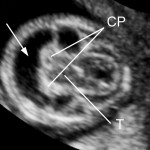

There is one single ventricular cavity (arrow); on its floor the fused choroid plexuses and thalami are seen. This fetus had associated trisomy 13 and an enlarged nuchal translucency that are better appreciated in the interactive volume. VISUOG I Lecture
Agenesis of corpus callosum (complete) I back to top I Index

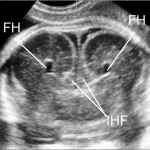
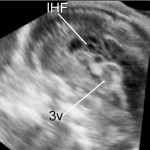
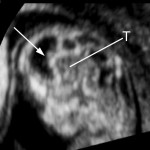
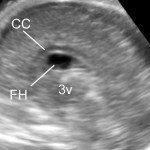
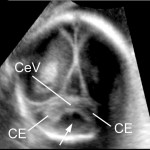
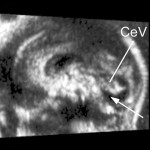
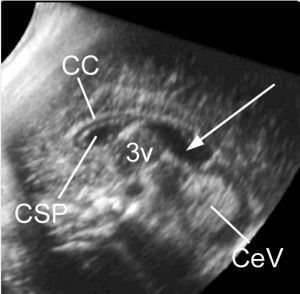
Axial view: The frontal horns are more distant than normal, the cavum septi pellucidi is not present and in its position only a distended interhemispheric fissure is seen. There is a slight enlargement of the atria. The increased separation between the frontal horns and the enlargement of the atria result in a tear-shaped configuration of the ventricle. Coronal view. The frontal horns (FH) are more distant than normal and have a typical ‘comma’ shaped appearance. The interhemispheric fissure (IHF) is distended and the two cerebral hemispheres are separated without any intervening corpus callosum. The sagittal view shows that above the area of the third ventricle (3v) the complex formed by the corpus callosum and cavum septi pellucidi is absent and replaced by the fluid contained into the interhemispheric fissure. VISUOG I Lecture
Partial agenesis of corpus callosum I back to top I Index


Abbreviations: 3v, third ventricle; At, atria; B, body of lateral ventricle; CC, corpus callosum; Ce, cerebellum; CeV, cerebellar vermis; CM, cisterna magna; CP choroid plexus; CSP, cavum septi pellucidi; FH, frontal horns, OH, occipital horns; TH, temporal horns),
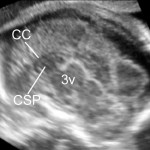
In the axial view and in the coronal view the brain appears unremarkable, with a seemingly normal cavum septi pellucidi. Only in the sagittal view the anomaly can be clearly demonstrated. The cavum septi pellucidi and the underlying cavum septi pellucidi are short and do not arch entirely over the cavity of the third ventricle.
Agenesis of the septum pellucidum I back to top I Index


On the axial view and in the coronal view the cavity and leaves of the cavum septi pellucidi are not demonstrated and the frontal horns are centrally fused; mild ventriculomegaly is also present. Conversely, the sagittal view is misleading because with this approach the fused frontal horns mimic a normal cavum septi pellucid. The corpus callosum appears normal as well. VISUOG I Lecture
Blake’s pouch cyst I back to top I Index


Axial view: The fourth ventricle seems to communicate with the cisterna magna through a small hourglass shaped opening. The sagittal view is the most informative one : the cerebellar vermis appears intact and is slightly rotated superiorly, with fluid interposed between it and the brain stem (arrow). VISUOG Lecture
Megacisterna magna I back to top I Index
The cisterna magna is enlarged but the cerebellum appears intact. VISUOG Lecture
3v, third ventricle; 4v, fourth ventricle; CC, corpus callosum; CE, cerebellar hemispheres; CeV, cerebellar vermis; CM, cisterna magna; CSP, cavum septi pellucidi; FH, frontal horns, T tentorium cerebelli; TH, temporal horns
Dandy-Walker Malformation I back to top I Index
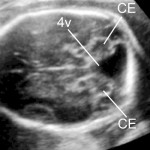

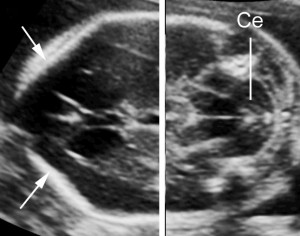
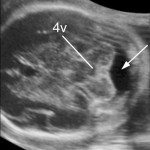
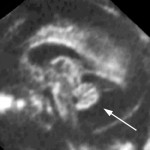
Axial view: The posterior fossa is occupied by a cystic structure with a well defined wall that arises from the fourth ventricles and spreads the cerebellar hemispheres apart. Although this approach is not sufficient for s specific differential diagnosis, the V-shaped appearance of the cyst dissecting in between the cerebellar hemispheres is strongly suggestive of Dandy-Walker malformation. The coronal view confirms the presence of increased fluid into the cisterna magna (arrow), but also indicates that the cerebellar vermis is present. The sagittal view is the most useful approach for a specific diagnosis: The posterior fossa is distended by a fluid accumulation; the cerebellar vermis is rotated superiorly; hypoplasia is inferred by the small dimensions and by the absence of the common landmarks, the triangular shape of the fourth ventricle and the main fissures. Note the high riding tentorium. VISUOG I Lecture
Vermian hypoplasia I back to top I Index

Axial view: The entire cerebellum appears of small size, there is a square-shaped fluid collection within the cerebellar hemispheres in the position normally occupied by the vermis, and the cisterna magna is not increased in size. The sagittal view provides the most relevant information for the diagnosis: The cerebellar vermis is rotated superiorly, very small and lacking the normal anatomic landmarks. VISUOG I Lecture
Arterio-venous malformation I back to top I Index


Arteriovenous malformation with aneurysmatic enlargement of the vein of Galen. Axial view: Color Doppler demonstrates a large vessel in the posterior third of the midline. Sagittal view: Abnormal vessel arising from the circle of Willis feed a very large vein of Galen that typically does not enter into the straight sinus, but is confluent with the falcine sinus; the superior sagittal sinus is enlarged. VISUOG
3v, third ventricle, CSP, cavum septi pellucidi; FS falcine sinus, PCA, pericallosal artery; SSS superior sagittal sinus, VG, vein of Galen
Intracranial hemorrhage grade IV I back to top I Index


The ventricles are enlarged and have an echogenic lining. A large blood clot is seen floating in one lateral ventricle. A cyst with an irregular lining (arrow) is seen in the periventricular area, indicating parenchymal involvement. VISUOG
Cavum veli interpositi I back to top I Index
The cavum veli interposition is a small anechoid area is seen posterior to the splenium of the corpus callosum in the area of the quadrigeminal cistern. It is difficult to differentiate between a cavum Vergae or a small cyst of the quadrigeminal cistern. However, all these conditions are without clinical implications.
What is Pocket Brain? I back to top I Index
Pocket Brain is a web-based, interactive ultrasound atlas of normal and abnormal fetal brain development. It can be viewed on any current internet-connected smartphone, tablet or computer, no installation required. Simply tap on any image to open a volume. Then scroll through the volumes by sliding with your finger (or mouse). Double-click to magnify (or to go back to normal size).
Pocket Brain also links to pertinent ISUOG’s Visual Encyclopedia (VISUOG) entries and selected ISUOG online lectures and publications.
Click here to view a short video of how to use Pockt Brain on a smartphone.
Index I back to top
- Normal brain
- Normal spine
- Spina bifida
- Ventriculomegaly
- Anencephaly
- Holoprosencephaly
- Agenesis of the corpus callosum
- Agenesis of the septum pellucidum
- Blake’s pouch cyst
- Megacisterna magna
- Dandy-Walker malformation
- Vermian hypoplasia
- Intracranial hemorrhage (IV)
- Cavum veli interpositi
References I back to top
- ISUOG CNS Guidelines 2007
- How do we do it: 3D brain, Pilu et al, UOG 2007
- Fetal brain VR, Tutschek and Pilu, UOG 2009
Acknowledgements
We are grateful to the following colleagues who kindly contributed translations for this site: Dr. Monica Cruz-Lemini, Mexico; Dr. Frederic Chantraine, Liege, Dr. K.Y. Leung, Hong Kong. What is Pocket Brain? I How to I Index I References I EN – DE – IT – ES – FR – RU – CN
Normal brain at midgestation: axial views
At, atria; B, body of lateral ventricle; CC, corpus callosum; Ce, cerebellum; CeV, cerebellar vermis; CM, cisterna magna; CP choroid plexus; CSP, cavum septi pellucidi; FH, frontal horns, OH, occipital horns; TH, temporal horns
The two sections shown above, the transthalamic and the transcerebellar view, constitute the brain screening exam. Further views are part of the extended fetal neurosonogram. ISUOG CNS Screening Guidelines I Lecture
Normal brain: coronal views (back to top)
Normal brain at midgestation: sagittal views (back to top)
At, atria; B, body of lateral ventricle; CC, corpus callosum; Ce, cerebellum; CeV, cerebellar vermis; CM, cisterna magna; CP choroid plexus; CSP, cavum septi pellucidi; FH, frontal horns, OH, occipital horns; TH, temporal horns
Normal spine I back to top I Index
Normal spine at midgestation: Sagittal view demonstrating the ossification centers of the spine, the integrity of the neural canal and the spinal cord. VISUOG I Lecture
Isolated ventriculomegaly I back to top I Index
Ventriculomegaly (VM) can accompany different brain pathologies. Isolated VM is a diagnosis of exclusion. The arrows indicate the distended lateral ventricles. VISUOG I Lecture
Anencephaly (late first trimester) I back to top I Index
The calvarium is absent and distorted brain tissue (arrow) is seen arising from the skull base and floating in the amniotic fluid. VISUOG
Spina bifida I back to top I Index
Myelomeningocele in a midtrimester fetus (sagittal view): In the sacral area the neural canal is open and communicates with a septated cystic mass (arrow); the spinal cord can be seen extending much lower than usual reaching the level of the defect. VISUOG I Lecture
Myelocele in a midtrimester fetus in sagittal view: In the sacral area the neural tube is open and exposed to the amniotic cavity without an interposing cystic structure. The sagittal plane demonstrates that the spinal cord reaches the level of the defect. VISUOG I Lecture
Arnold-Chiara malformation (cranial signs of spina bifida) I back to top I Index
Arnold-Chiari malformation in a fetus with open spina bifida: There is frontal bossing (also referred to as lemon sign) (arrows); the cerebellum (Ce) is poorly delineated because of the absence of fluid in the cisterna magna (also referred to as banana sign).VISUOG I Lecture
Holoprosencephaly, alobar (13 weeks‘ fetus) I back to top I Index
There is one single ventricular cavity (arrow); on its floor the fused choroid plexuses and thalami are seen. This fetus had associated trisomy 13 and an enlarged nuchal translucency that are better appreciated in the interactive volume. VISUOG I Lecture
Agenesis of corpus callosum (complete) I back to top I Index
Axial view: The frontal horns are more distant than normal, the cavum septi pellucidi is not present and in its position only a distended interhemispheric fissure is seen. There is a slight enlargement of the atria. The increased separation between the frontal horns and the enlargement of the atria result in a tear-shaped configuration of the ventricle. Coronal view. The frontal horns (FH) are more distant than normal and have a typical ‘comma’ shaped appearance. The interhemispheric fissure (IHF) is distended and the two cerebral hemispheres are separated without any intervening corpus callosum. The sagittal view shows that above the area of the third ventricle (3v) the complex formed by the corpus callosum and cavum septi pellucidi is absent and replaced by the fluid contained into the interhemispheric fissure. VISUOG I Lecture
Partial agenesis of corpus callosum I back to top I Index
Abbreviations: 3v, third ventricle; At, atria; B, body of lateral ventricle; CC, corpus callosum; Ce, cerebellum; CeV, cerebellar vermis; CM, cisterna magna; CP choroid plexus; CSP, cavum septi pellucidi; FH, frontal horns, OH, occipital horns; TH, temporal horns),
In the axial view and in the coronal view the brain appears unremarkable, with a seemingly normal cavum septi pellucidi. Only in the sagittal view the anomaly can be clearly demonstrated. The cavum septi pellucidi and the underlying cavum septi pellucidi are short and do not arch entirely over the cavity of the third ventricle.
Agenesis of the septum pellucidum I back to top I Index
On the axial view and in the coronal view the cavity and leaves of the cavum septi pellucidi are not demonstrated and the frontal horns are centrally fused; mild ventriculomegaly is also present. Conversely, the sagittal view is misleading because with this approach the fused frontal horns mimic a normal cavum septi pellucid. The corpus callosum appears normal as well. VISUOG I Lecture
Blake’s pouch cyst I back to top I Index
Axial view: The fourth ventricle seems to communicate with the cisterna magna through a small hourglass shaped opening. The sagittal view is the most informative one : the cerebellar vermis appears intact and is slightly rotated superiorly, with fluid interposed between it and the brain stem (arrow). VISUOG Lecture
Megacisterna magna I back to top I Index
The cisterna magna is enlarged but the cerebellum appears intact. VISUOG Lecture
3v, third ventricle; 4v, fourth ventricle; CC, corpus callosum; CE, cerebellar hemispheres; CeV, cerebellar vermis; CM, cisterna magna; CSP, cavum septi pellucidi; FH, frontal horns, T tentorium cerebelli; TH, temporal horns
Dandy-Walker Malformation I back to top I Index
Axial view: The posterior fossa is occupied by a cystic structure with a well defined wall that arises from the fourth ventricles and spreads the cerebellar hemispheres apart. Although this approach is not sufficient for s specific differential diagnosis, the V-shaped appearance of the cyst dissecting in between the cerebellar hemispheres is strongly suggestive of Dandy-Walker malformation. The coronal view confirms the presence of increased fluid into the cisterna magna (arrow), but also indicates that the cerebellar vermis is present. The sagittal view is the most useful approach for a specific diagnosis: The posterior fossa is distended by a fluid accumulation; the cerebellar vermis is rotated superiorly; hypoplasia is inferred by the small dimensions and by the absence of the common landmarks, the triangular shape of the fourth ventricle and the main fissures. Note the high riding tentorium. VISUOG I Lecture
Vermian hypoplasia I back to top I Index
Axial view: The entire cerebellum appears of small size, there is a square-shaped fluid collection within the cerebellar hemispheres in the position normally occupied by the vermis, and the cisterna magna is not increased in size. The sagittal view provides the most relevant information for the diagnosis: The cerebellar vermis is rotated superiorly, very small and lacking the normal anatomic landmarks. VISUOG I Lecture
Arterio-venous malformation I back to top I Index
Arteriovenous malformation with aneurysmatic enlargement of the vein of Galen. Axial view: Color Doppler demonstrates a large vessel in the posterior third of the midline. Sagittal view: Abnormal vessel arising from the circle of Willis feed a very large vein of Galen that typically does not enter into the straight sinus, but is confluent with the falcine sinus; the superior sagittal sinus is enlarged. VISUOG
3v, third ventricle, CSP, cavum septi pellucidi; FS falcine sinus, PCA, pericallosal artery; SSS superior sagittal sinus, VG, vein of Galen
Intracranial hemorrhage grade IV I back to top I Index
The ventricles are enlarged and have an echogenic lining. A large blood clot is seen floating in one lateral ventricle. A cyst with an irregular lining (arrow) is seen in the periventricular area, indicating parenchymal involvement. VISUOG
Cavum veli interpositi I back to top I Index
The cavum veli interposition is a small anechoid area is seen posterior to the splenium of the corpus callosum in the area of the quadrigeminal cistern. It is difficult to differentiate between a cavum Vergae or a small cyst of the quadrigeminal cistern. However, all these conditions are without clinical implications.
What is Pocket Brain? I back to top I Index
Pocket Brain is a web-based, interactive ultrasound atlas of normal and abnormal fetal brain development. It can be viewed on any current internet-connected smartphone, tablet or computer, no installation required. Simply tap on any image to open a volume. Then scroll through the volumes by sliding with your finger (or mouse). Double-click to magnify (or to go back to normal size).
Pocket Brain also links to pertinent ISUOG’s Visual Encyclopedia (VISUOG) entries and selected ISUOG online lectures and publications.
Click here to view a short video of how to use Pockt Brain on a smartphone.
Index I back to top
- Normal brain
- Normal spine
- Spina bifida
- Ventriculomegaly
- Anencephaly
- Holoprosencephaly
- Agenesis of the corpus callosum
- Agenesis of the septum pellucidum
- Blake’s pouch cyst
- Megacisterna magna
- Dandy-Walker malformation
- Vermian hypoplasia
- Intracranial hemorrhage (IV)
- Cavum veli interpositi
References I back to top
- ISUOG CNS Guidelines 2007
- How do we do it: 3D brain, Pilu et al, UOG 2007
- Fetal brain VR, Tutschek and Pilu, UOG 2009
Acknowledgements
We are grateful to the following colleagues who kindly contributed translations for this site: Dr. Monica Cruz-Lemini, Mexico; Dr. Frederic Chantraine, Liege, Dr. K.Y. Leung, Hong Kong.